


"Rare" Career Threatening Back Injury for MLB Superstar Mike Trout
Are you serious?



The Los Angeles Angels, and fans of Major League Baseball were dealt some seriously bad news yesterday regarding one of the games superstars.
It was released that Mike Trout, arguably the best offensive player of the last decade and a 3-time AL MVP, was diagnosed with a “rare” back condition labelled T5 Costovertebral Dysfunction that has kept him on the DL since July 12 and will significantly shorten the rest of his 2022 season.
If it has been documented what the mechanism of his costovertebral dysfunction is, I haven’t seen it, however more troubling perhaps than his recent history, which suggests neurological stagnation and biological accommodation.
Trout who will soon turn 31 years old has only played 168 games combined over the last three seasons (keep in mind one of those seasons, 2020 was shortened to 60 games due to COVID-19, however Trout only played 53 of those), and hasn’t really played close to a full season since 2016, which suggests he has been accommodating for quite some time, long before his most recent setback. In that time, he has had to overcome a torn calf muscle which occurred while running the bases in the early part of the 2021 season and shut him down for the remainder. He has also felt with nagging oblique issues and nagging back pain at various points in his career.
What is Costovertebral Dysfunction?
I’m not sure how rare costovertebral dysfunction truly is because no evidence exists as to the incidence of this condition. Anecdotally, I can say that I see a handful of cases per year of irritated thoracic spines in athletes where the source of that discomfort can be traced to the costovertebral joint, through palpation and physical examination, although the potential for other findings does exist.
Relevant Anatomy

Trout’s injury is at the level of T5, which is highlighted in green in the above picture from Complete Anatomy, whereby you can visualize the fifth rib on both sides of the ribcage articulating into the thoracic spine at the level of the fifth vertebra. As you can also observe in the model above, the level of the fifth vertebra would be inter scapular when landmarked on the body from an external perspective. This delineates the true mid back as the thoracic vertebra at the upper region (T1) is shaped and behaves similarly to the cervical spine and the lower thoracic vertebra (T10-12) start to become more lumbar spine like in their shape and behaviour.

The head of the corresponding rib articulates into the sides of both the fourth and fifth vertebral bodies with the corresponding T4 disc in between. The head of the rib is held in place by the Radiate ligament which can be considered the articular capsule of the costovertebral joint as this ligament spans directionally all around the rib head and therefore creates the space within which the rib can move during both breathing and thoracic spine movement.
Important Anatomical Relationships
Again, in reference to the model above and those structures highlighted in green, it is important to note some important anterior anatomical relationships that are relevant to this type of injury. First off, all structures highlighted in green have a connective tissue basis. At a cellular level this is extremely important as this creates a microscopic linkage between structures as their composition is similar, the behaviour of the tissue will be similar and their response to loading (and overloading) will be similar. From this anterior view it is fairly easy to see that the costovertebral articular capsule has an evident flow of tissue directionality and composition into the intervening vertebral disc of T4. The outer annular fibres of the vertebral disc are connective tissue based and have a radial (circular) orientation to them. It is clear that this creates an anatomical and behavioural linkage between the costovetebral joint and the vertebral disc.
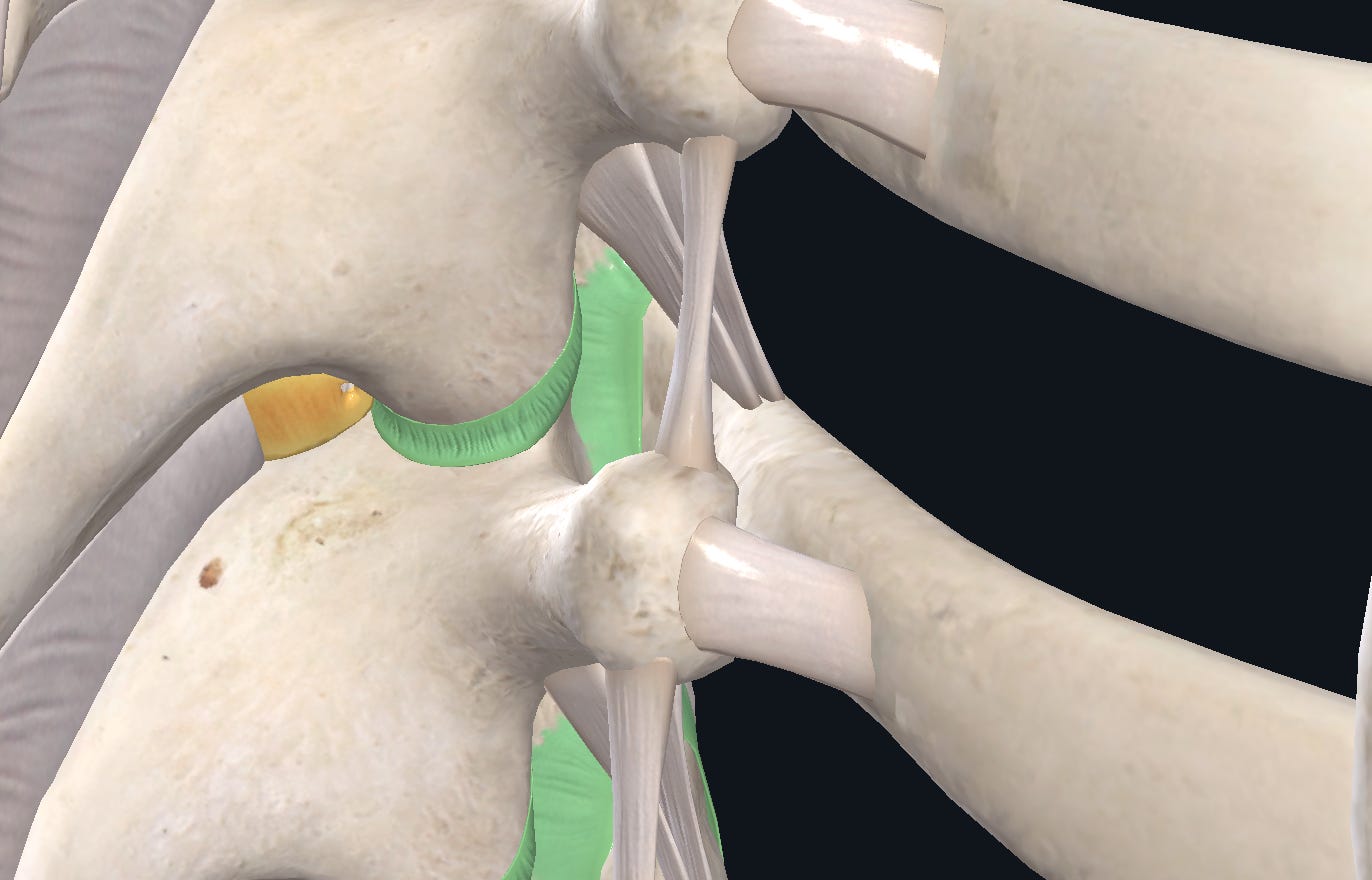
From a posterior view seen in the above model (again highlighted in green), it is important to note an anatomical relationship between the thoracic spine facet joint at capsule T4/5 and the costovertebral joint capsule of T5. Again, the similarities of both being connective tissue, and sharing a direction, gives indication of micro (cellular) and macro (anatomical, behavioural) linkages.
The Thoracic Spine
From an evolutionary perspective the thoracic spine is quite important in that it has been "around” the longest, from the time of quadrapedalism. As such it is considered a primary curve and the subsequent selection for the lumbar spine and pelvis, and the cervical spine were an adaptation to the change to bipedalism and the kyphotic curve of the thoracic spine.
To this point, it should be largely understood that the thoracic spine does possess a large capacity for flexion and to a lesser extent but still important extension. Extension will be less than flexion due to the primary nature of the thoracic curve as well as the fact that the ribcage will inherently limit a large amount of extension of the thoracic spine.
When looking at rotation and lateral flexion specifically of the thoracic spine the movements are maximal at the levels between T4-9, but realistically are quite small (4-6 degrees per segment) and are often contributed to by motion of the lumbar spine.
This leads us to make one of the most important conclusions of thoracic spine mechanics:
Due to the primary nature of the thoracic curve and the relevant anatomical linkages, flexion and extension are fundamental movements, both segmentally and globally, of this region of the spine.
At FRS, we have placed this in such high importance that it is a rule that governs the system, and how to both assess and train the thoracic spine (and the cervical and lumbar spine).
Rotation and lateral flexion of the spine, although important for spinal adaptability in movement are not fundamental. They are created secondarily and emerge based on the underlying capacity of the spine to flex and extend both segmentally and globally.
Injury Speculation
At Absolute, we have no knowledge of the background historical data leading up to Trout’s injury, however we can speculate on what might have occurred (and is occurring).
Baseball is a highly rotational sport, will both major skills of the game, throwing and hitting, revolving around the ability of the athlete to effectively and. efficiently rotate through the trunk (amongst other joints).
Trout is one of the most dangerous hitters in the game. Without going into the mechanics of hitting, it is very plain to see in the clip below that during the initial loading phase, his spine will rotate backwards, in his case to the right, and then will rotate again to the left, this time with high velocity during the launch phase into ball contact and follow through. It is also important to note that at ball contact Trout’s spine is rotating and lateral flexing to the right while being in flexion. It is safe to say that hitting the ball with power requires a large capacity of spinal behaviour both in movement and strength.
Management of This Injury
To this point the management of this injury has followed the traditional sports injury model. This consists of rest and corticosteroid injection. Highly unlikely to deal with the potential underlying behaviours of the internal ecosystem and how it emerges behaviour externally.
At Absolute, the management of this injury would be multifaceted in an attempt to create simultaneous effects, both on the underlying tissues and the way they interact to create emergent powerful, yet skilled movement.
This starts at the joint level, whereby the creation of capsular space, in the fundamental motions of the thoracic spine (flexion/extension) would be paramount to changing the outward behaviour of the thoracic facet joints, allowing more space and time for the thoracic spine to create secondary rotation and lateral flexion. When specifically done at the level of T4/5 through direct anatomical linkages this would impact the costovertebral joint at T5, also allowing for more space and time during movement.
Creating capsular space has direct affects on afferent flow to the CNS, and is a major conduit to modifying behavioural output. This would be important to Trout as this would allow him to have more information available to him and this be more adaptable at the plate, depending on the type of pitch that is thrown to him.
Simultaneous training inputs to the deeper spinal tissues, to improve their physiological capacity to do work over sustained time frames would also be important in this case.
Lastly, training the prime movers of the spine (obliques, rectus abdominis, lats etc) to display reactive strength and speed strength (see upcoming article in Establishing Point B) would create the optimal level of thoracic performance for any athlete involved in rotational sports.
Follow Along
At Absolute, we will definitely be monitoring the progress of Trout and his return to Major League Baseball.
You can follow along too through his social media