
Hamstring Injury Management: The Intermediate Phase
Utilizing the Internal Isometric Continuum to generate a conjugation of treatment and training effects during the intermediate phase.


Case Overview
A few weeks ago, there were a multitude of hamstring injuries that presented in the clinic, all as a result of increasing training volume with arguably a lack of appropriate ecological training leading up to the injury.
One such case occurred in a sprinter making the transition from indoor training to outdoor training. During one session, he felt the left hamstring seize up. He sought treatment five days after the injury still very sore, with very limited range of motion and the ability to fully bear weight through that leg during the gait cycle, which is an important outcome to achieve if the athlete is unable to do so.
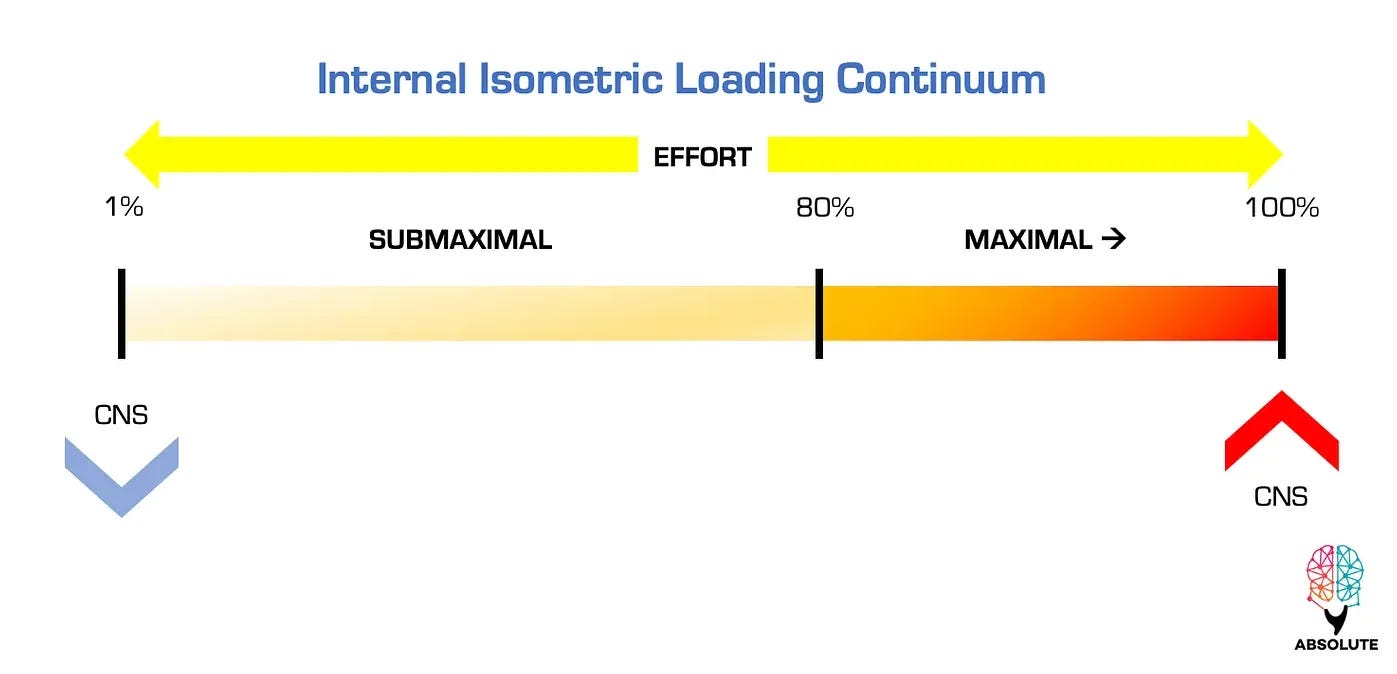
Due to the injury, there were both local and global effects within the neural network of absolute strength, which can become major limiting factors to the progression toward Point B as the management of the injury progresses. As a result, much of the initial management included easy entry points to the neural network as a way to create repetitive stimulation to engage all layers. Using the Internal Isometric Continuum (IIC) repeated use of isoramping inputs throughout the hamstring as well as positional isometrics (PIMAs) in non-affected ranges at the maximal sustainable effort level as determined by the athlete were used to continually prompt the network.
Neural Damping & Network Stimulation
The goals of this initial management were to engage the network repeatedly to encourage re-connections amongst the nodes in each layer, and doing so at a level that the network currently “understands”. Keep in mind the injury creates a damping effect within the network whereby the CNS attempts to prevent excessive neural excitation and minimize nodal instability through the layers with the goal of returning to some level of homeostasis. Although well-intentioned, a more optimal state of the network cannot occur without the network being stimulated to try and minimize this damping effect.

Criteria for Progression into Intermediate Phase
The clinical signs of progression into the intermediate phase are straightforward. The athlete must possess full and painless passive and active linear range of motion of both the hip and the knee. In addition, the ability to fully engage the whole hamstring to the highest effort level possible during isoramping contractions is required as this shows that the neural network has been stimulated to a level that is requisite to eliminate any neurological spasm and guarding but also to a level that allows for the progression of hamstring outputs during the intermediate phase.
Considerations for Point B
As the athlete moves forward in the training progressions, it is now necessary to consider all elements of Point B and where there may be limitations in each capacity so that they can begin to be trained in this phase. At this point, it is necessary to build a better biological foundation that the nervous system can output into. The intermediate phase of the program is usually the longest and the most dense from a programming perspective as it requires the highest frequency of inputs (Bulgarian method) to create the environment for tissue change.

Soft Tissue Healing Phases (Jarvinen et al.)
One of the most influential papers published in the sports medicine literature regarding the topic of soft tissue healing post-injury was written by Jarvinen et al. In the article, the authors outline the specific details of tissue regeneration from directly after injury to return to status. It is an extremely useful resource when dealing with soft tissue injuries and the timelines of cellular processes to aid the practitioner in making decisions regarding the appropriate inputs during each time frame.
From the article a soft tissue injury will go through three stages:
Destruction Phase: occurs directly post-injury force and is characterized by the inflammatory process and the formation of a hematoma between areas of the tissue that have been damaged as a result of the mechanism.
As discussed in the initial article on this case this phase is also associated with both local and global effects as governed by the CNS which are neurological mechanisms designed to protect the tissue during this phase.
Repair Phase: this is the intermediate phase whereby the immune system is further activated to initiate the breakdown of the injured tissue and the subsequent regeneration of the myofibers. There is also the production of a connective tissue scar that creates a bridge between the two sides of the injury. Ultimately, the production and management of the scar has a direct correlation to the eventual quality of the repair of the tissue. As practitioners, this is the primary goal of this phase. Using progressive inputs that create directional forces across the bridge, and loading the tissue at length, to length, and through length are the stresses necessary to build the foundation of tissue repair and stiffness.
Remodeling Phase: this is the final phase and is distinguished by the reorganization of the tissue architecture and the eventual recovery of the functional capacities of the tissue.
Using the Internal Isometric Continuum
Again, in this intermediate phase, the Internal Isometric Continuum is very useful to help create the necessary inputs to influence the biological organization and architecture of the tissue. Creating directionality and initial stiffness is paramount to appropriate tissue healing post-injury. This is done using submaximal repeated yielding PAILs efforts to the tolerance of the tissue. The impetus with these inputs is to maximize the directional loading over the maximal amount of time within the session. In addition for those in the clinic, the use of FR manual techniques is paramount to guide the tissue in the ways of healing and reorganization.
Practical Application for this Case
The athlete in this case had two in-clinic days, while the rest of the week was spent performing training inputs on his own.
Here is the breakdown of all tissue-specific inputs as well as other training inputs.
Conjugate in the Clinic
Keep reading with a 7-day free trial
Subscribe to Absolute: The Art and Science of Human Performance to keep reading this post and get 7 days of free access to the full post archives.