
Tightness: An Indicator of Abnormal Connective Tissue Architecture
Athlete Tightness: The Dre Greenlaw Case



Tightness: A Leading Indicator
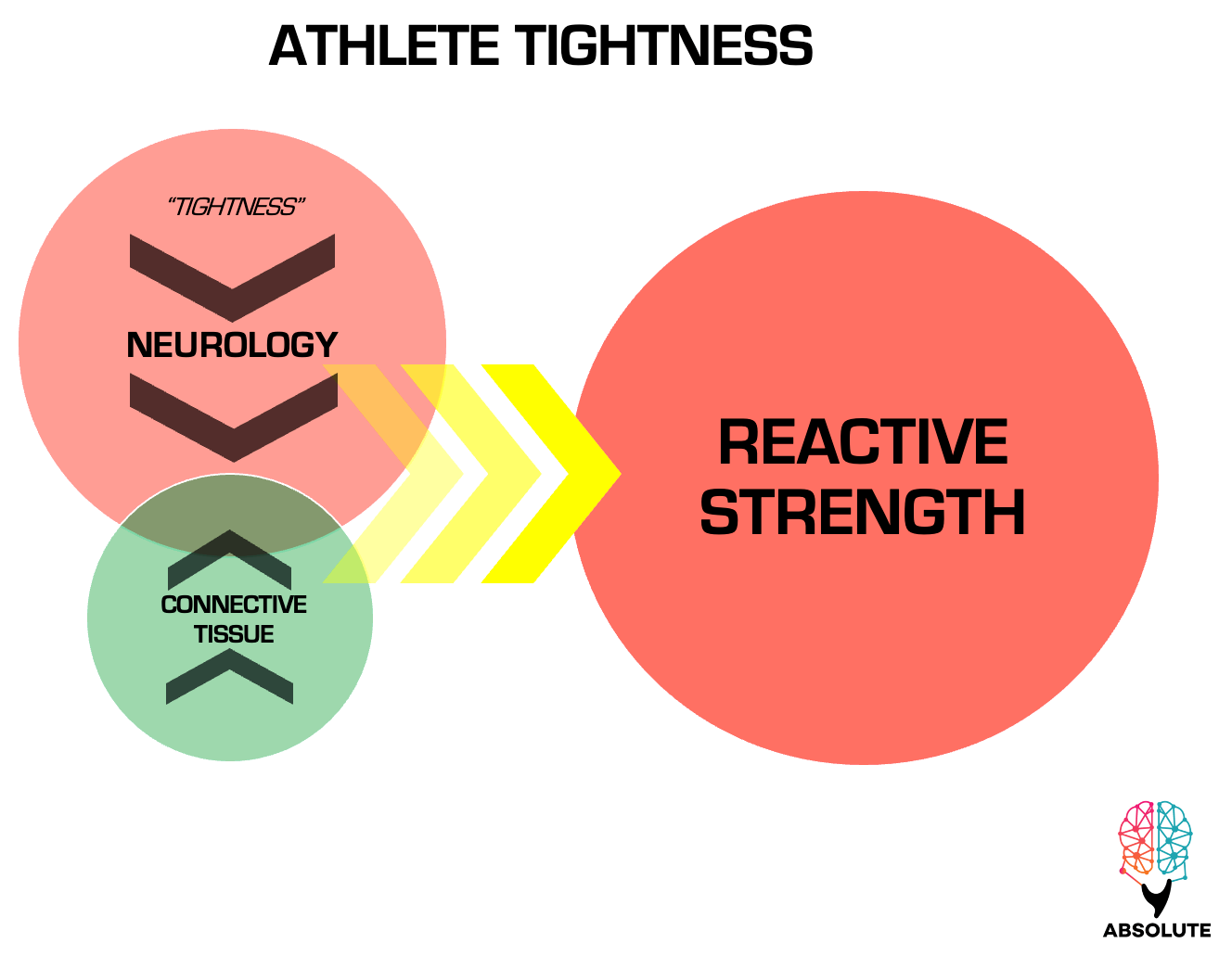
When an athlete complains of or exhibits tightness—such as in Dre Greenlaw’s Tightness Case—it serves as a leading indicator for us as strength practitioners to take immediate action. High-level athletes like Greenlaw possess the neurological capacity to maximally compress their absolute strength network, pushing their connective tissues to the very edge of chaos during explosive collisions or rapid changes in direction scenarios. The unfortunate part for these dynamic athletes is that their neurology can put them in force transmission scenarios that push past the edge of chaos, where the force exceeds the tissue's ability to effectively transmit it and reactive strength injury occurs.
The same neurological ability that is the hallmark of the NFL’s most violent and explosive athletes—the best players, tragically, predisposes them to reactive strength injuries, particularly when the connective tissue architecture becomes abnormal. The transition from normal to abnormal connective tissue is common during the demands of an NFL in-season schedule and lack of optimal connective tissue-specific training or, as in Greenlaw’s case, following an Achilles tendon rupture from the previous year.
The NFL's Reactive Strength Problem Showcased in Super Bowl 58

Dre Greenlaw Achilles tendon reactive strength injury.
Leading Indicators = Information Flow
As practitioners, we must recognize tightness as information flow that the athlete needs to be shut down from violent, change-of-direction force output scenarios and physically assessed for abnormal connective tissue architecture using tissue tension assessment.1
Leading indicators are metrics that provide critical information flow, helping to predict future events—in this case, reactive strength injuries—and conditions, such as abnormal connective tissue architecture. Tightness, in this context, indicates that the connective tissue architecture may have undergone maladaptive changes, behaving abnormally and requiring immediate intervention to prevent further injury—as the nervous system is giving the athlete more top-down support, which the athlete is verbally telling us is tightness.

The Elephant in the Room: Outdated MRI Feedback Only Loop
In 2024, practitioners have the ability to objectively assess connective tissue architecture behavior in just minutes. Yet many NFL clinics remain stuck in outdated, inefficient practices. Unfortunately, most athletic trainers and clinical staff either lack a clear understanding of tightness and reactive strength or the palpatory skills required to manually assess connective tissue behavior—skills developed through consistent hands-on practice, not illogical bullshit like Theraguns.
Instead, franchise clinics continue to rely primarily on MRI machines—a process that moves at the pace of a leisurely elephant’s stroll. This outdated approach forces athletes to undergo imaging, requires radiologists to interpret the results, and delays actionable decisions until clinical staff can review the findings—this is a frustrating process for all parties involved.
For athletes like Dre Greenlaw, who operate on tight weekly cycles (7 days), this slow feedback loop is simply impractical. In leagues like the NHL, and NBA, where schedules are even more compressed and road trips are regular, the inefficiency becomes even more amplified. To effectively treat and train modern high-performance athletes within optimal timeframes, accurate information must flow at the speed of the demands—not lag behind them. Unfortunately, the current MRI model fails to deliver either speed or the specific information flow we are practitioners need.

We Don’t Need MRIs to Act
During our recent presentation at the FRS Summit on a return-to-performance case we successfully managed, we shared findings from the DOHA Agreement Meeting—experts in hip joint clinical management—who concluded that imaging is often unnecessary for effective clinical action. These insights align with Absolute’s belief: the outdated MRI feedback loop not only wastes time and resources but also perpetuates stagnation in sports medicine. Worse still, it fails to meet the needs of modern athletes, doing them a significant disservice in the pursuit of maximizing their athletic potential into reality.
Leading Indicators in Absolute’s Practice
In our extensive work with this athlete population, we educate all athletes that tightness is a clear signal for immediate tissue assessment.2 Similarly, we emphasize that closing-angle joint pain is abnormal and warrants immediate joint assessment. This is not new territory for us; we recognize that when working with athletes who possess both the neurology and psychology to push their biology beyond its loading limits, it’s essential to rely on simple but highly effective leading indicators like tightness and closing angle joint pain. These indicators help us determine when to pull athletes from the level of competition to address and resolve joint dysfunction or abnormal connective tissue at the level of adaptation before it escalates into a reactive strength injury.
The Neurology Won’t Stop Scaling: Good!
We must emphasize that the athlete’s neurology won’t stop scaling—nor do we want it to, as we are using training to augment it.3 At Absolute, our ethos is to utilize both treatment and training to bring the athlete’s absolute potential into reality—hence the name Absolute. The standard is to develop the athlete into a physical state (Point B) where they can generate performances at levels never seen before, breaking through stagnation and redefining what’s possible. Why else are we here if not to push these boundaries???
Understand: it is this relentless ethos of pushing for growth that has rewarded us time and time again—doing anything else would be nonsensical.
Why Tightness Indicates Abnormal Connective Tissue
Tightness exists because the mechanoreceptors embedded in abnormal connective tissue feed disorganized or maladaptive information into the neurology.4 The CNS, in turn, interprets this information as a vulnerability in the connective tissue architecture and responds with a top-down protective strategy: increasing neural output into the surrounding musculature to stabilize the area and reduce the perceived risk of further injury.
This top-down support—manifesting as 'tightness'—is not a mistake but a reflexive response of the neurology to protect connective tissue architecture that is compromised. The tightness limits the tissue's ability to lengthen, reducing range of motion and thereby minimizing the forces transmitted through the tissue to prevent further damage/reactive strength injury.
Key Insight in Context of Reactive Strength
Keep reading with a 7-day free trial
Subscribe to Absolute: The Art and Science of Human Performance to keep reading this post and get 7 days of free access to the full post archives.